Books
The Association for Applied Psychophysiology and Biofeedback (AAPB) published Don Moss and my Primer of Biofeedback. It was published in Taiwan and soon in Mexico.
AAPB will also publish Khazan, Shaffer, Moss, Lyle, and Rosenthal’s Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.) in September 2023.
Journal Articles
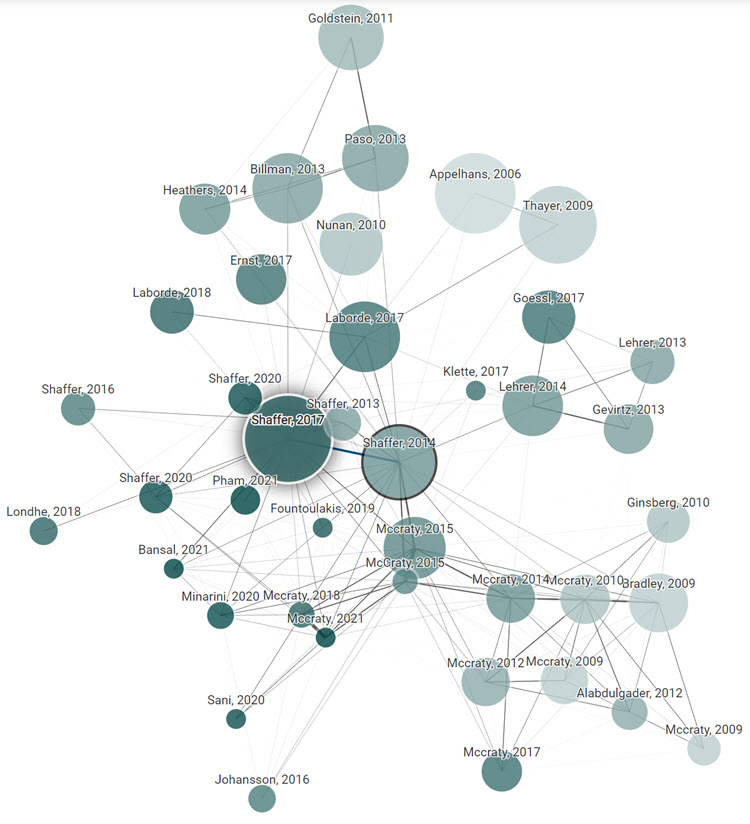
Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2014.01040. 835 citations. Altmetric Attention Score 64.
Heart rate variability (HRV), the change in the time intervals between adjacent heartbeats, is an emergent property of interdependent regulatory systems that operate on different time scales to adapt to challenges and achieve optimal performance. This article briefly reviews neural regulation of the heart, and its basic anatomy, the cardiac cycle, and the sinoatrial and atrioventricular pacemakers. The cardiovascular regulation center in the medulla integrates sensory information and input from higher brain centers, and afferent cardiovascular system inputs to adjust heart rate and blood pressure via sympathetic and parasympathetic efferent pathways. This article reviews sympathetic and parasympathetic influences on the heart, and examines the interpretation of HRV and the association between reduced HRV, risk of disease and mortality, and the loss of regulatory capacity. This article also discusses the intrinsic cardiac nervous system and the heart-brain connection, through which afferent information can influence activity in the subcortical and frontocortical areas, and motor cortex. It also considers new perspectives on the putative underlying physiological mechanisms and properties of the ultra-low-frequency (ULF), very-low-frequency (VLF), low-frequency (LF), and high-frequency (HF) bands. Additionally, it reviews the most common time and frequency domain measurements as well as standardized data collection protocols. In its final section, this article integrates Porges’ polyvagal theory, Thayer and colleagues’ neurovisceral integration model, Lehrer et al.’s resonance frequency model, and the Institute of HeartMath’s coherence model. The authors conclude that a coherent heart is not a metronome because its rhythms are characterized by both complexity and stability over longer time scales. Future research should expand understanding of how the heart and its intrinsic nervous system influence the brain.
Shaffer, F., & Ginsberg, J. P. (2017). An Overview of heart rate variability (HRV) metrics and norms. Frontiers in Public Health: Family Medicine and Primary Care.
https://doi.org/10.3389/fpubh.2017.00258. 1907 citations. Altmetric Attention Score 155.
Healthy biological systems exhibit complex patterns of variability that can be described by mathematical chaos. Heart rate variability (HRV) consists of changes in the time intervals between consecutive heartbeats called interbeat intervals (IBIs). A healthy heart is not a metronome. The oscillations of a healthy heart are complex and constantly changing, which allow the cardiovascular system to rapidly adjust to sudden physical and psychological challenges to homeostasis. This article briefly reviews current perspectives on the mechanisms that generate 24 h, short-term (~5 min), and ultra-short-term (<5 min) HRV, the importance of HRV, and its implications for health and performance. The authors provide an overview of widely-used HRV time-domain, frequency-domain, and non-linear metrics. Time-domain indices quantify the amount of HRV observed during monitoring periods that may range from ~2 min to 24 h. Frequency-domain values calculate the absolute or relative amount of signal energy within component bands. Non-linear measurements quantify the unpredictability and complexity of a series of IBIs. The authors survey published normative values for clinical, healthy, and optimal performance populations. They stress the importance of measurement context, including recording period length, subject age, and sex, on baseline HRV values. They caution that 24 h, short-term, and ultra-short-term normative values are not interchangeable. They encourage professionals to supplement published norms with findings from their own specialized populations. Finally, the authors provide an overview of HRV assessment strategies for clinical and optimal performance interventions.
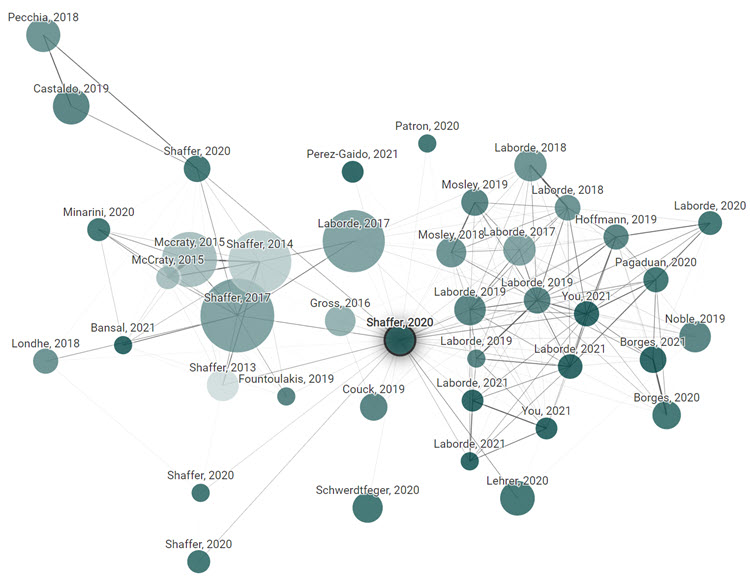
Shaffer, F., & Meehan, Z. M. (2020). A practical guide to resonance frequency assessment for heart rate variability biofeedback. Frontiers in Neuroscience. https://doi.org/10.3389/fnins.2020.570400. 12 citations. Altmetric Attention Score 31.
Heart rate variability (HRV) represents fluctuations in the time intervals between successive heartbeats, which are termed interbeat intervals. HRV is an emergent property of complex cardiac-brain interactions and non-linear autonomic nervous system (ANS) processes. A healthy heart is not a metronome because it exhibits complex non-linear oscillations characterized by mathematical chaos. HRV biofeedback displays both heart rate and frequently, respiration, to individuals who can then adjust their physiology to improve affective, cognitive, and cardiovascular functioning. The central premise of the HRV biofeedback resonance frequency model is that the adult cardiorespiratory system has a fixed resonance frequency. Stimulation at rates near the resonance frequency produces large-amplitude blood pressure oscillations that can increase baroreflex sensitivity over time. The authors explain the rationale for the resonance frequency model and provide detailed instructions on how to monitor and assess the resonance frequency. They caution that patterns of physiological change must be compared across several breathing rates to evaluate candidate resonance frequencies. They describe how to fine-tune the resonance frequency following an initial assessment. Furthermore, the authors critically assess the minimum epochs required to measure key HRV indices, resonance frequency test-retest reliability, and whether rhythmic skeletal muscle tension can replace slow-paced breathing in resonance frequency assessment.
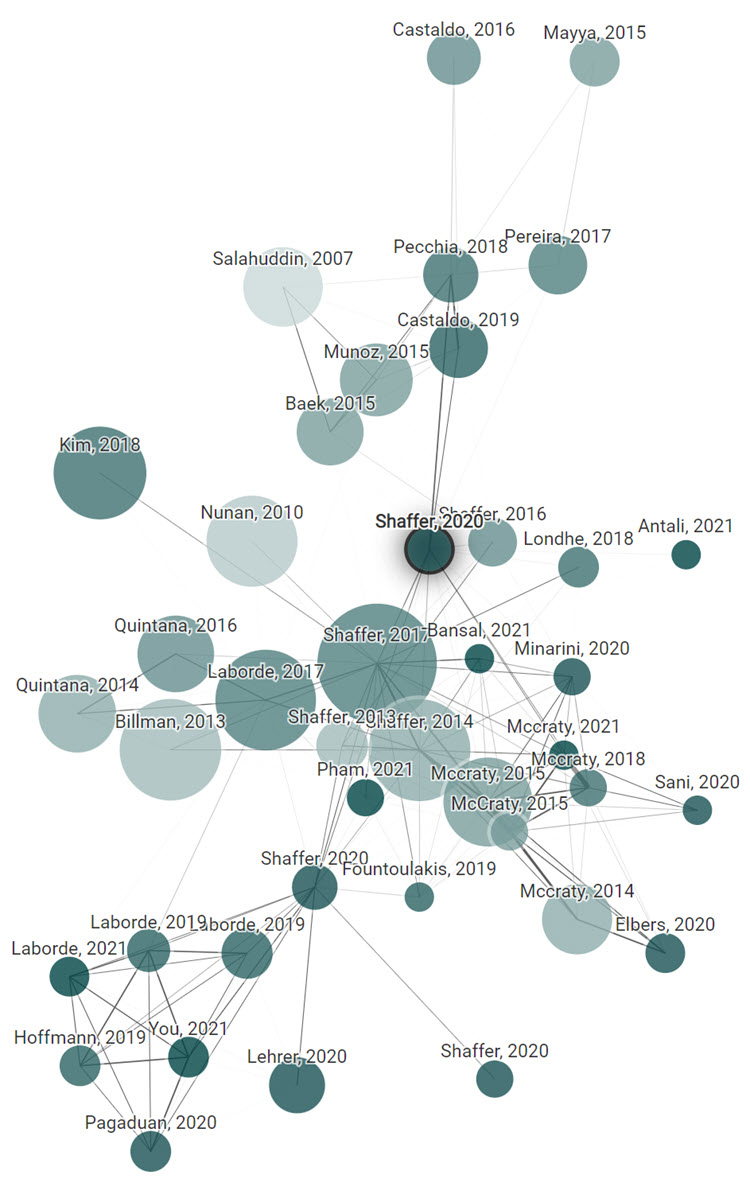
Shaffer, F., Meehan, Z. M., & Zerr, C. L. (2020). A critical review of ultra-short-term heart rate variability norms research. Frontiers in Neuroscience. https://doi.org/10.3389/fnins.2020.594880. 8 citations. Altmetric Attention Score 1.
Heart rate variability (HRV) is the fluctuation in time between successive heartbeats and is defined by interbeat intervals. Researchers have shown that short-term (∼5-min) and long-term (≥24-h) HRV measurements are associated with adaptability, health, mobilization, and use of limited regulatory resources, and performance. Long-term HRV recordings predict health outcomes heart attack, stroke, and all-cause mortality. Despite the prognostic value of long-term HRV assessment, it has not been broadly integrated into mainstream medical care or personal health monitoring. Although short-term HRV measurement does not require ambulatory monitoring and the cost of long-term assessment, it is underutilized in medical care. Among the diverse reasons for the slow adoption of short-term HRV measurement is its prohibitive time cost (∼5 min). Researchers have addressed this issue by investigating the criterion validity of ultra-short-term (UST) HRV measurements of less than 5-min duration compared with short-term recordings. The criterion validity of a method indicates that a novel measurement procedure produces comparable results to a currently validated measurement tool. We evaluated 28 studies that reported UST HRV features with a minimum of 20 participants; of these 17 did not investigate criterion validity and 8 primarily used correlational and/or group difference criteria. The correlational and group difference criteria were insufficient because they did not control for measurement bias. Only three studies used a limits of agreement (LOA) criterion that specified a priori an acceptable difference between novel and validated values in absolute units. Whereas the selection of rigorous criterion validity methods is essential, researchers also need to address such issues as acceptable measurement bias and control of artifacts. UST measurements are proxies of proxies. They seek to replace short-term values which, in turn, attempt to estimate long-term metrics. Further adoption of UST HRV measurements requires compelling evidence that these metrics can forecast real-world health or performance outcomes. Furthermore, a single false heartbeat can dramatically alter HRV metrics. UST measurement solutions must automatically edit artifactual interbeat interval values otherwise HRV measurements will be invalid. These are the formidable challenges that must be addressed before HRV monitoring can be accepted for widespread use in medicine and personal health care.
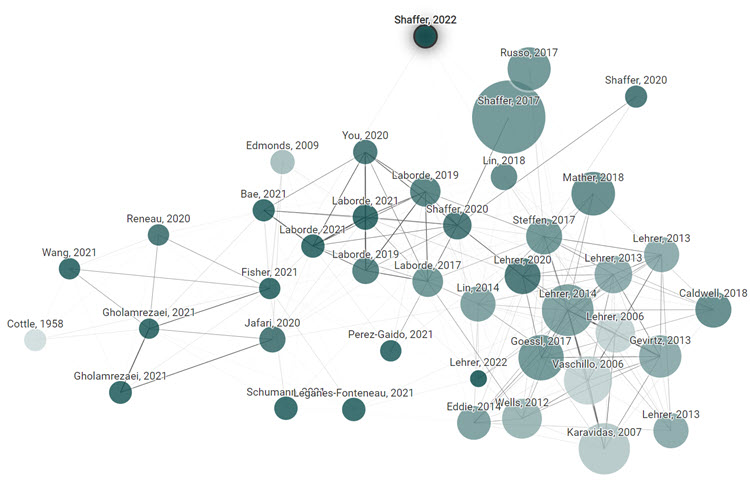
Shaffer, F., Moss, D., & Meehan, Z. M. (2022). Rhythmic skeletal muscle tension increases heart rate variability at 1 and 6 contractions per minute. Appl Psychophysiol Biofeedback.
https://doi.org/10.1007/s10484-022-09541-7. 1 citation.
Breathing at the resonance frequency (~ 6 breaths per min) produces resonance effects on baroreflex gain, blood pressure, vascular tone, and therapeutic benefits. Evgeny Vaschillo and Paul Lehrer have emphasized that the stimulation frequency is critical for producing resonance effects in the cardiorespiratory system. Although clinicians overwhelmingly use paced breathing to increase HRV, other promising methods exist. Vaschillo, Lehrer, and colleagues have shown that presenting non-respiratory stimulation at 0.1 Hz—pictures with an emotional valence or rhythmical muscle tensing—amplifies oscillations in heart rate, blood pressure, and vascular tone. Participants in the present study included 49 undergraduate students randomly assigned to one of six different orders of 5-min trials of 1, 6, and 12 muscle contractions per min (cpm), separated by 3-min buffer periods intended to minimize carryover. This randomized controlled trial replicated the Vaschillo et al. (Psychophysiology 48:927–936, 2011. https://doi.org/10.1111/j.1469-8986.2010.01156.x) finding that 6-cpm RSMT can produce a PkFreq of ~ 0.10 Hz, similar to 6-bpm RF breathing. RSMT at 1 and 6 cpm increased five time-domain metrics (HR Max–HR Min, RMSSD, SDNN, TI, and TINN), one frequency-domain metric (LF power), and three non-linear metrics (D2, SD1, SD2) significantly more than RSMT at 12 cpm. There were no differences between 1 and 6 cpm on these measures. The 1-cpm rate
(~ 0.02 Hz) may have stimulated the hypothesized vascular tone baroreflex between 0.02 and 0.055 Hz. RSMT at 1 or 6 cpm provides clients with an alternative exercise for increasing HRV for patients who find slow-paced breathing challenging or medically unsafe.
Shaffer, F., & Meehan, Z. M. (2022). An undergraduate program with heart: Thirty years of Truman HRV research. Appl Psychophysiol Biofeedback. https://doi.org/10.1007/s10484-022-09543-5. 0 citations.
This article celebrates the contributors who inspired Truman’s heart rate variability (HRV) research program. These seminal influences include Robert Fried, Richard Gevirtz, Paul Lehrer, Erik Peper, and Evgeny Vaschillo. The Truman State University Applied Psychophysiology Laboratory’s HRV research has spanned five arcs: interventions to teach diaphragmatic breathing, adjunctive procedures to increase HRV, HRV biofeedback (HRVB) training studies, the concurrent validity of ultra-short-term HRV measurements, and rhythmical skeletal muscle tension strategies to increase HRV. We have conducted randomized controlled trials, primarily using within-subjects and mixed designs. These studies have produced eight findings that could benefit HRVB training. Effortful diaphragmatic breathing can lower end-tidal CO2 through larger tidal volumes. A 1:2 inhalation-to-exhalation (I/E) ratio does not increase HRV compared to a 1:1 I/E ratio. Chanting “om,” listening to the Norman Cousins relaxation exercise, and singing a fundamental note are promising exercises to increase HRV. Heartfelt emotion activation does not increase HRV, enhance the effects of resonance frequency breathing, “immunize” HRV against a math stressor, or speed HRV recovery following a math stressor. Resonance frequency assessment achieved moderate (r = 0.73) 2-week test-reliability. Four weeks of HRVB training increased HRV and temperature, and decreased skin conductance level compared with temperature biofeedback training. Concurrent-validity assessment of ultra-short-term HRV measurements should utilize rigorous Pearson r and limits of agreement criteria. Finally, rhythmical skeletal muscle tension can increase HRV at rates of 1-, 3-, and 6-cpm. We describe representative studies, their findings, significance, and limitations in each arc. Finally, we summarize some of the most interesting unanswered questions to enable future investigators to build on our work.
Meehan, Z. M., & Shaffer, F. (2023). Adding core muscle contraction to wrist-ankle rhythmical skeletal muscle tension increases respiratory sinus arrhythmia and low-frequency power.
Paced breathing and rhythmical skeletal muscle tension (RSMT) at an individual’s resonance frequency (~6 breaths or contractions per min) can stimulate the arterial and vascular tone baroreflexes. Lehrer (2022) has explained that the stimulation rate is important, not the modality. Early RSMT protocols differed in the muscles recruited and whether legs were crossed or uncrossed. France and colleagues (2006) studied the contraction and relaxation of the abdomen, buttocks, and legs with legs crossed. Lehrer and colleagues (2009) and Vaschillo and colleagues (2011) investigated wrist-ankle contraction with the legs uncrossed. Whereas core muscle RSMT with crossed legs and wrist-ankle RSMT with uncrossed legs produced resonance effects, researchers have not directly compared the effect of these exercises on respiratory sinus arrhythmia (RSA) and low-frequency (LF) power. The current within-subjects experiment investigated whether crossing the legs and recruiting core muscles (e.g., gluteus maximus and rectus abdominis) can enhance wrist-ankle RSMT effects on RSA and LF power. We compared 6-cpm wrist-ankle RSMT (ankles uncrossed) with 6-cpm wrist-core-ankle RSMT (ankles crossed) and a control condition in which participants sat quietly (ankles uncrossed) without performing RSMT. Based on the French and colleagues (2006) findings, we predicted that 6-cpm wrist-core-ankle RSMT would produce greater heart rate (HR), HR Max-HR Min, and LF power than the other conditions. We selected these dependent variables because HR and HR Max-HR Min provide evidence that RSMT has stimulated the baroreflex, whereas LF power measures the degree to which resonance effects have occurred within the 0.04-0.15-Hz range, targeted in HRV biofeedback. We randomly assigned 35 participants to one of six different orders of conditions, each separated by 3-min buffer periods. The experimental findings supported our predictions. Both RSMT conditions produced greater HR, HR Max-HR Min, and LF power than the control condition. Wrist-core-ankle yielded greater HR and HR Max-HR Min than wrist-ankle RSMT. Since we cannot quantify the contribution of leg position to our results, future research should compare wrist-ankle and wrist-core-ankle RSMT with legs crossed. The practical implication for HRV biofeedback training is that wrist-core-ankle RSMT with legs crossed may more powerfully stimulate the baroreflex than wrist-ankle RSMT with legs uncrossed.
Shaffer, F., & Moss, D. (2023). Review of I. Z. Khazan (2019), Biofeedback and Mindfulness in Everyday Life: Practical Solutions for Improving Your Health and Performance.
Dr. Inna Khazan is the preeminent authority on integrating biofeedback with mindfulness. She wrote Biofeedback and Mindfulness in Everyday Life for biofeedback clients, individuals seeking self-improvement, clinicians, performance coaches, and students. Part I, Physiological Principles, describes the major biofeedback modalities, breathing physiology, and heart rate variability. Part II, Mindfulness, reviews the Foundations of Mindfulness, Mindfulness Meditation, Mindfulness-Based Skills, and Compassion and Self-Compassion. Part III, Applications to Common Challenges, addresses Sleep, Stress and Performance, Anxiety and Fear, Anger, Interpersonal Communication, Pain, Sadness and Depression, and Shame and Guilt. Two appendices contain Meditation Scripts and a Sample List of Biofeedback Devices. Khazan masterfully explains the science supporting biofeedback, mindfulness-based interventions, and self-regulation. Biofeedback and Mindfulness in Everyday Life provides a step-by-step guide for building resilience and emotional flexibility and addressing challenges like anxiety, depression, and pain.

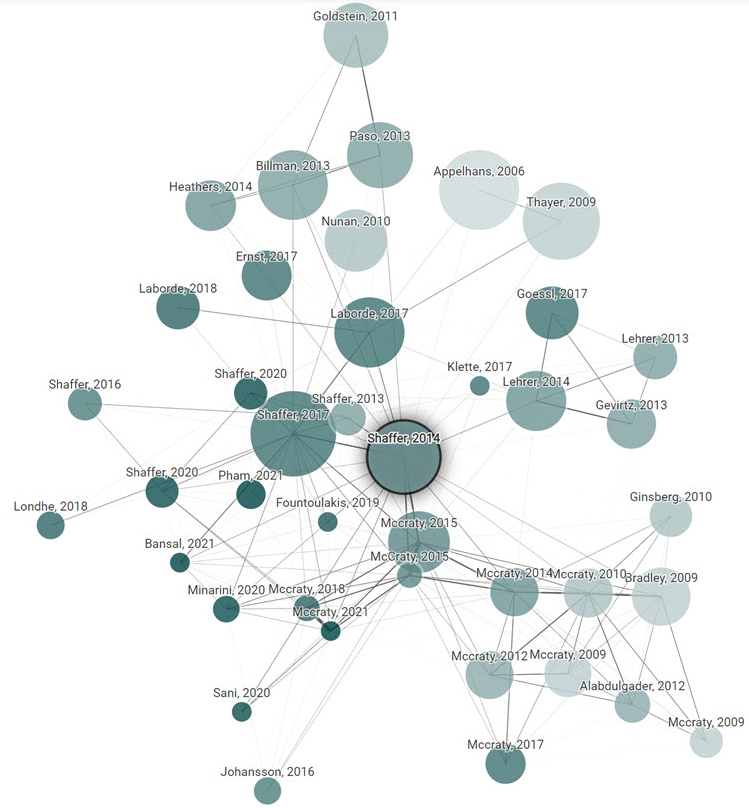
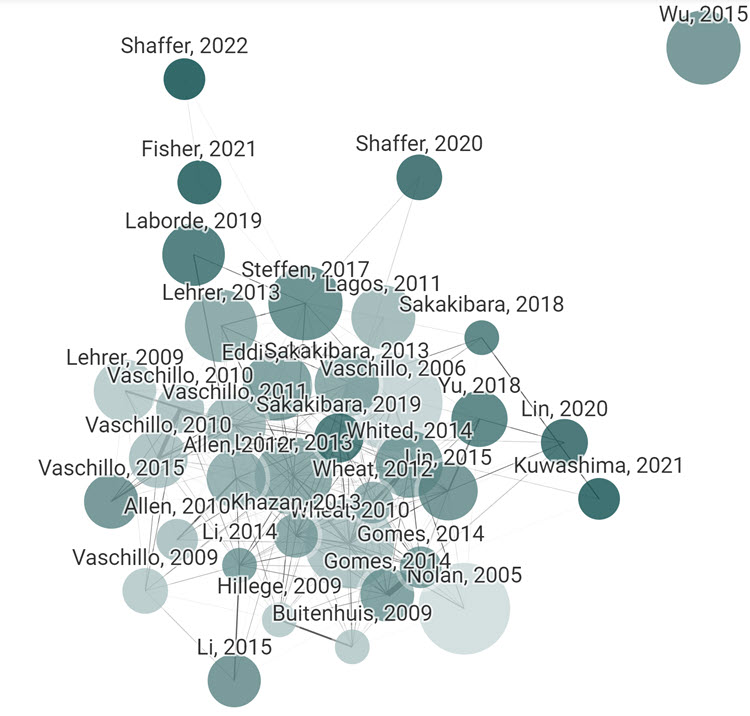
Connected Papers generated the graphs that illustrate the connections of articles to our origin article.
“How does it work? To create each graph, we analyze an order of ~50,000 papers and select the few dozen with the strongest connections to the origin paper. In the graph, papers are arranged according to their similarity. That means that even papers that do not directly cite each other can be strongly connected and very closely positioned. Connected Papers is not a citation tree. Our similarity metric is based on the concepts of Co-citation and Bibliographic Coupling. According to this measure, two papers that have highly overlapping citations and references are presumed to have a higher chance of treating a related subject matter. Our algorithm then builds a Force Directed Graph to distribute the papers in a way that visually clusters similar papers together and pushes less similar papers away from each other. Upon node selection we highlight the shortest path from each node to the origin paper in similarity space. Our database is connected to the Semantic Scholar Paper Corpus (licensed under ODC-BY). Their team has done an amazing job of compiling hundreds of millions of published papers across many scientific fields.”